What your team gets
Linda does the dialing; your people get the signal. Every program feeds the same four outputs.
Reports and alerts from every interaction
Every call becomes a clear report, and alerts flag the interactions that need staff follow-up — delivered instantly by SMS and email.
A complete profile for every patient or member
Their data (via CSV or API), full history of activity with Linda, every alert and report — plus a place for your staff to add notes.
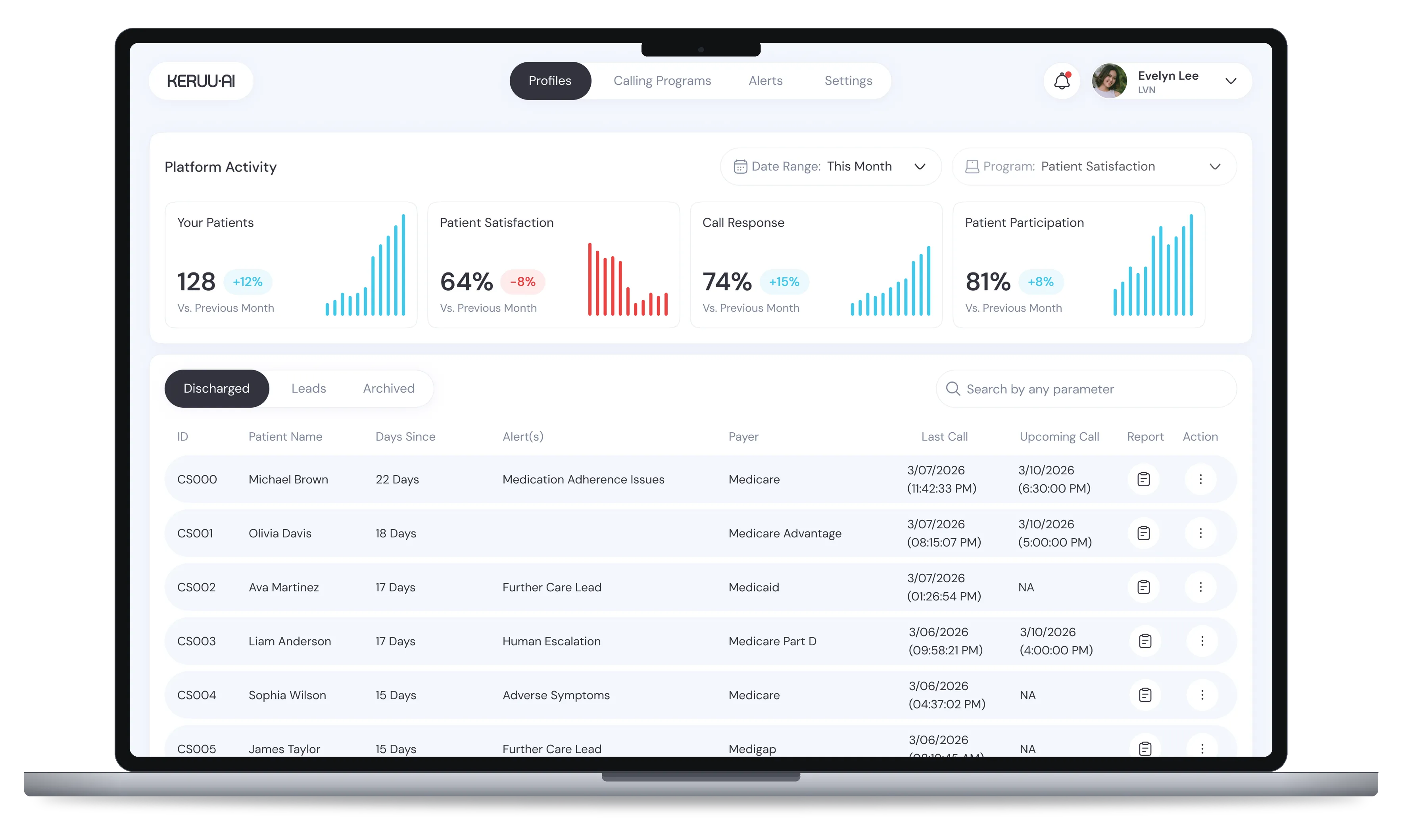
A real-time dashboard with high-level KPIs
See Linda’s activity across your entire patient or member pool at a glance, and track the numbers that matter.
Full visibility into every program
View your active call programs, the questions each one covers, and the sequence strategy — number of attempts, time between calls, and calling approach.